Diagnostic & Hospital Equipments
Open MRI Machine: Top Systems Compared Before You Invest

If you are a healthcare provider considering an investment in MRI, you know what’s at stake. You want clear images, a comfortable patient experience, and a reasonable overall cost of ownership. This guide to Open MRI machine will help you keep a balance between relief from claustrophobia and diagnostic quality. Read on to compare top machines before you invest.
What Is an Open MRI Machine?
The open MRI machine has a left side, a right side, or both, or no sides at all. Unlike the typical closed-bore models, which enclose you in a small, tunnel-like tube. “Open” can be one of several things: two pillars, four-sided access, or a C-shaped magnet.
Basically, open designs versus closed designs allow easier access to the patient and a more comfortable experience for the patient; however, many low-field systems compromise some image resolution for that comfort.
This structural difference solves the main worry of claustrophobic patients who would otherwise decline or battle through needed diagnostic scans. “Open” relates to access to the patient and does not mean there is no magnetic field. Still, these systems use strong magnetic fields and radiofrequency pulses to produce diagnostic images.
Healthcare providers usually get constant questions on what an open MRI machine is and whether the image quality is the same as with the traditional model.
Key Considerations When Choosing an Open MRI Machine
Choosing an appropriate MRI system involves thorough considerations, some of which are:
Patient comfort
The reduction of claustrophobia as well as easy access to the scanner for all patients (especially for children, old people, and those with phobias) are the most important features. In addition, design matters, as does noise and lighting, and even seating choices.
Image quality and field strength
High field strength provides sharper images and faster scan times, but this can increase claustrophobia. The trade-offs are worth considering because open systems produce lower magnetic fields than closed ones.
Procedural flexibility
Upright positions, diverse weights, and coexistence with implants are other important factors. Certain open MRI scanners allow a patient to sit upright or can accommodate a larger body habitus or patients with implants that might not fit in a standard MRI machine.
Throughput and uptime
Facility managers must also weigh throughput, system uptime, maintenance requirements, total cost of ownership, and space constraints.
Is There an Alternative to an MRI Scan If You Are Claustrophobic?
Healthcare professionals know that some patients may not tolerate a conventional MRI, even with comfort measures such as music, mirrors, or sedatives. Alternatives are available for people with extreme claustrophobia; however, there are some clinical considerations.
CT allows faster scanning and better patient compliance, but it exposes the patient to ionizing radiation and might not show the same level of soft tissue characterization. Ultrasound is excellent for some superficial structures, but it cannot penetrate bone or air to image the body internally.
Also, some centers have special MRI protocols for nervous patients: shorter sequences and open configuration systems can combine with tilted table positions to remove the sense of enclosure.
Although sedation regimens administered by anaesthesiologists help some patients to undergo standard MRI studies, this modality is associated with further hazards and extra cost.
What is the difference between an open MRI and traditional MRI?
Knowing the basic differences between open and traditional closed-bore MRI machines allows buyers and vendors to choose the right one. Open MRI units generally have lower field strengths, such as between 0.35 Tesla and 1.2 Tesla, which influence the duration of the scan and image resolution.
Closed-bore MRI machines operate at much higher field strengths (usually 1.5T or 3T) and produce images much faster with higher quality, particularly on advanced protocols such as neuro, oncology, and MS (musculoskeletal).
The patient experience is night and day between the two configurations. Traditional narrow bores can be terrifying for those who suffer from claustrophobia, while open models allow patients to have natural light and feel less confined. ‘
Open MRI Machine: The Top Models
Several manufacturers offer open MRI systems designed to maximize patient comfort and produce quality imaging. Each has strengths and weaknesses; however, the choice depends on the clinical scenario, the level of patient comfort, and the budget. The options include the following:
Hitachi Oasis (1.2T) Open MRI Machine
The Hitachi Oasis is the high end of true open MRI technology and is the highest field strength available in a truly open configuration. It offers unprecedented open access on four sides with its breakthrough 2-pillar design. Also, the SPACE allows a truly open, spacious environment for patients.
Design Features:
- True open architecture; 4 sides open (access)
- 1.2 Tesla field strength
- Wider bore of 65 cm
- Advanced gradient coil technology
Advantages:
- Best image quality within the true-open category
- Good for routine body as well as ortho and spine work
- It seats larger patients, up to approximately 500 lbs.
- There is a huge reduction in the comfort complaints of claustrophobia.
Disadvantages:
- More expensive initial cost relative to low-field open systems
- Higher maintenance costs when compared with permanent magnet systems.
- Do not use for advanced neuro protocols with a 3T requirement.
Application:
Excellent for institutions that want to provide comfortable patient conditions and high-sensitivity images for orthopaedics and general examinations. The Hitachi Oasis is for a patient who needs diagnostic quality approximating conventional 1.5T systems.
Siemens Magnetom C (0.35T) Open MRI Machine
The Siemens Magnetom C demonstrates “open” MRI in a way that is suitable for the patient. It uses a C-shape magnet configuration that provides maximum access to the patient and still reduces patient anxiety. The system performs well in pediatric imaging and for centers dealing with highly claustrophobic patients.
Design Features:
- The C-shaped open magnet design
- 0.35 Tesla field strength
- Cryogen-Free Permanent Magnet Technology
- Small footprint ideal for smaller healthcare providers
Advantages:
- Excellent patient comfort, with an open view on three sides
- Child-friendly environment – with parents sitting near them during the scans
- Lower cost for acquisition and installation
- Small running costs attributable to the cryogen-free design
- Much quieter operation than the high-field systems
Disadvantages:
- Lower fields mean longer scans.
- The depth of the images produced by a high-field system is much higher.
- Restricted advanced neuro/vascular protocol facility
Application:
Pediatric imaging centers; community hospitals with limited budgets; and sites that cater to an increasingly claustrophobic patient base. The Siemens Magnetom C permits acceptable diagnostic quality for a large volume of standard examinations while focusing on the patient experience.
GE Signa HDxt or Optima (1.5T Wide Bore)
Even though they are not open systems, the GE wide-bore models lie somewhere in between the traditional bore length and open MRI machines. The 1.5T systems offer the same diagnostic power as the technology that patients expect from Intermountain Healthcare, now with enhanced patient comfort.
Design Features:
- 70 cm wide bore opening
- 1.5 Tesla field strength
- Full complement of advanced clinical applications
- Works with traditional MRI coils and other accessories
Advantages:
- High-resolution imaging equivalent to traditional 1.5T systems
- Full compatibility with standard clinical protocols
- It’s significantly more comfortable than the traditional 60 cm bore machines.
- Proven service infrastructure
Disadvantages:
- They’re not truly open and can cause panic attacks in claustrophobic individuals.
- Larger patients may have a tight fit.
- Does not allow full upright positioning
Application:
An institution requiring 1.5T imaging capability with enhanced patient comfort. These systems are for locations where image quality cannot be compromised for patient comfort and for diverse patient populations, such as larger body habitus.
A Practical Decision-Making Framework for Facilities
Healthcare organizations can use the framework below when acquiring MRI technology.
Step 1: Determine the Patient Population
Start with your most frequent exams. Orthopedic, neurological, pediatric, body. Sports medicine centers have different demands than children’s hospitals, and community hospitals that cater to an aging population have challenges compared to those of academic medical centers.
Step 2: Evaluate Patient Comfort Goals
For high-volume claustrophobic patient centers, true open systems should be emphasized, while centers dealing with cooperative patients may emphasize image quality parameters over comfort features.
Step 3: Assess Imaging Needs
Consider system features and specific sequences or protocols by your key service lines (clinical needs). A few specialized neurology applications do require 3T field strength, and the open designs are not suitable for those, no matter what the comfort factor advantages.
Step 4: Check the Total Cost
Estimate comprehensive costs such as hardware capital investment, site preparation and installation, ongoing maintenance, service contracts, and operational expenditures. The total cost of ownership of open MRI machines is higher than that of closed units and depends on magnet type, maintenance needs, and upgrades.
Step 5: Organize Space, Installation, and Training
Evaluate building infrastructure (e.g., electrical, shielding, floor loading, area). Factor in the schedule for staff training and workflow adaptation for delays in time to productivity for post-installation.
Step 6: Factor in Service and Upgrade Roadmap
Assess the quality of manufacturer support, the potential for upgrades, and the viability of a long-term relationship. Cryogen-free variants require simple maintenance, whereas superconducting designs enable field upgrades but require cryogen management.
Open MRI Machine: Investment Factors
The financial review of MRI acquisitions is more complicated than the simple purchase price and includes many factors that affect the total investment. They include:
Initial purchase price
The initial purchase price is only one factor; the cost of installation, site preparation, and infrastructure modifications are other costs to consider, too.
Field strength vs. image resolution needs
Field strength determines the potential image resolution, but the operational and maintenance costs increase proportionally with the strength of the system.
Open versus broad-bore versus true open trade-off
The decision to have an open, broad-bore, or narrow-bore scanner is a balancing act between patient comfort, diagnostic ability, and facility economics.
Features of patient comfort
Noise suppression, lighting, built-in entertainment facilities, and sound all add high cost, but how a patient reacts is different.
Maintenance and response times
Costs of maintenance also differ between permanent magnet and superconducting systems, with cryogen-free systems presenting a predictable ongoing cost.
Workflow-friendly
Workflow integration with traditional PACS, EMR, and scheduling systems has implications for workflow and should be considered.
Regulatory and safety aspects
Hospitals need to take this into account for patients with implants, devices, or special monitoring requirements.
Clinical and Operational Suggestions
To get an open MRI technology, focus on clinical procedures and operational workflows that boost patient comfort.
When dealing with patients who experience claustrophobia, combining open MRI machines with thorough information sessions before the procedure can ease their stress.
Healthcare providers should establish consistent methods such as facility walkthroughs, comprehensive explanations of what the procedure involves, and clear communication about what patients should expect.
For patients with claustrophobia, integrate open MRI systems with educational and comfort strategies.
Implement user-friendly support tools for positioning, and permit a family member or friend to stay with the patient during the scan if policies allow.
If there is a need for precise, high-field imaging, explore protocols that enhance both the speed and comfort of open MRI systems, or use dedicated high-field open scanners like the Hitachi Oasis for select cases only.
What’s the difference? Open MRI vs. True Open vs. Wide-Bore

Open MRI (patient comfort)
- True open: Maximum patient access with the widest comfort, usually with 0.35–1.2 T ranges; ideal for claustrophobic and some pediatric cases with compromises in speed and resolution.
- Wide-bore: about 70 cm, wider and more comfortable than traditional narrow bores, high-end imaging at 1.5T; still has walls, so some patients may feel claustrophobic and intimidated.
Near-term considerations
- Cryogen-free versions reduce operating costs and the complexity of maintenance.
- Phased upgrade flexibility: modularity allows customers to upgrade in phases to accommodate growth in demand or evolving protocols.
- Make sure to be PACS-compatible and IT-integrated to reduce workflow friction and maximize interoperability.
Clinical and operational advice (cont.)
- Pre-procedure education helps reduce anxiety.
- Use soothing environments: low lighting, soft music, and the patients have control of some aspects of the procedure.
- Combine the open MRI with seating for caregivers or family members to be present, if policy allows.
Read also: How Does an MRI Machine Work?
Final Thoughts on Open MRI Machine
The choice of an open MRI system involves trade-offs between patient comfort and the diagnostic requirements. So, healthcare providers should know their core patient base.
For a practice with very nervous or pediatric patients, open systems such as the Hitachi Oasis or Siemens Magnetom C are valuable solutions that reduce sedation.
An open or C-shaped magnet might be preferred for those with large populations of pediatric or claustrophobic patients. However, centers focused on high-resolution 1.5T imaging and that accommodate a wider variety of patients may choose a wide-bore, non-fully-open design.

Are you thinking of a knee replacement but don’t want surgery? Then this is for you. A knee cartilage repair without surgery remains an elusive goal in the field of orthopedics. Current non-operative therapies do not regenerate large amounts of hyaline cartilage tissue as surgical methods such as ACI or MACI do. Instead, these treatments focus on pain relief, enhanced function, and improved joint stability, especially in mild-to-moderate osteoarthritis or focal chondral lesions.
Here, you’ll find information on non-operative treatment and therapies for your knee. It will help you understand the options and develop a plan with your physical therapist.
What is Knee Cartilage Repair without Surgery?
It is when nonoperative care may complement or even precede surgery. The goal is to reduce pain, improve function, and slow the wear of knee cartilage.
How it works
Nonsurgical treatment of arthritis in the knee is to reduce inflammation, enhance joint lubrication, protect the knee, and support the cartilage. Treatments can be combined with a home exercise program and lifestyle measures to protect the joint. If symptoms worsen, the plan can be modified.
Expected symptom relief and typical regimen
Some people see relief within weeks, while others need several months of continued treatment. Treatments may include injections (when necessary), physical therapy, and lifestyle changes. Therapy may also include regular visits, exercise, or changes in diet.
Stem Cell Knee Injections
Stem cell injections for the knee are cells that may help repair or change the environment of the joint. These cells are injected into the knee to decrease inflammation and promote tissue health.
Types: Bone marrow-derived and adipose-derived
Bone marrow-derived stem cells are taken from your bone marrow and processed for injection. Adipose-derived stem cells are taken from the fat tissue and processed for use in the knee.
Purpose:
Inhibit inflammation
Support healing signals in the joint
Improve cartilage quality and function (Further study is needed)
Hyaluronic acid knee injections (lubricate joint and reduce stiffness)
Hyaluronic acid (HA) injections add a slippery fluid to the knee joint to improve lubrication and reduce friction.
Purpose:
HA acts as a lubricant and shock absorber
Helps the joint glide
Decrease stiffness
Increase range of motion
Dosage and viscosity:
Doses vary, with several injections a week or one high-dose injection
Viscosity is important. It may require a higher viscosity form of cream
The benefits:
Reduces pain during movement
Improve joint function for a period of weeks to months
Viscosupplementation Knee Cartilage Repair without Surgery
Viscosupplementation refers to the injection of hyaluronic acid into joints to improve joint viscosity. The two treatments are very similar but referred to slightly differently.
Time of relief: Most patients notice immediate relief after a few weeks to a few months. Some feel relief for much longer periods of time with activity modification and PT.
Prolotherapy Knee Cartilage Repair without Surgery
Prolotherapy involves small injections that stimulate the body’s healing response to strengthen ligaments and joint stability.
Injection targets:
Ligaments in the knee and areas believed to be loose or unstable. The goal is to improve the joint alignment and stress on the cartilage when moving.
Benefits
Could remove the micro-movements that cause cartilage irritation
It can supplement strengthening and PT by providing a more stable foundation for the knee.
Physical Therapy Knee Cartilage Repair without Surgery
Physical therapy is important in the non-surgical knee care program. It is not just about strengthening. It restores normal joint motion and reverses common biomechanical problems such as excessive knee valgus or foot pronation.
In addition, it improves neuromuscular control so that loads are evenly distributed into the joint.
The protocol usually begins with managing the pain with ice or gentle mobilization. Then move to closed-chain exercises such as mini-squats, step-ups, and open-chain strengthening and functional drills.
Purpose:
- To restore pain-free movement.
- Enhance range of motion.
- Build the muscles supporting the knee.
Typical protocols:
- A logical progression: Manage pain, move comfortably, load slowly.
- Add neuromuscular training to enhance knee tracking and stability.
- Use the imaging guide for progression when necessary.
Knee Muscle Strengthening
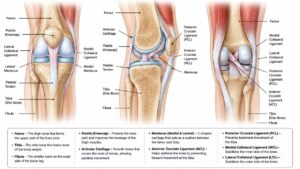
What muscle groups should I work on?
- The quadriceps, especially the vastus medialis
- Hamstring
- Hip abductors and the gluteal complex
- Calf muscles for ankle-knee synergism.
How does this reduce pressure in the cartilage?
- Strong muscles carry more load, and the cartilage is less directly loaded
- Improved knee alignment reduces uneven wear on the surface of the joint
- Lower-impact exercises for bad knees
- Low-impact exercises help keep the knee healthy
Examples:
- Swimming: Offers a full-body workout without stressing joints.
- Cycling: Use of stationary or road cycling
- Elliptical: Allows fluid motion with less impact on the knees
- Walking schedules: Slow progression on distance and speed
Knee Cartilage Diet
Nutrition only assists in the treatment of the joint environment and is not a medicine. A knee cartilage diet helps to reduce inflammation and the level of chronic low-grade inflammation that contributes to the progression of osteoarthritis.
The following foods are recommended:
- Foods high in omega-3 (fatty fish such as salmon, mackerel, sardines
- (Flaxseeds, chia seeds, walnuts)
- Color fruits and vegetables
- Make olive oil your main fat and eat lean protein (legumes and poultry).
- Limit processed foods, refined sugars, and too much saturated fat.
Here are some meal ideas:
- Breakfast: Greek yogurt with berries and flaxseed
- Lunch: Hefty salad with grilled salmon, mixed greens, chickpeas, olive oil/vinegar dressing
- Dinner: Stir-fried tofu, broccoli, peppers, brown rice, and ginger-garlic sauce
Weight Loss for Knee Pain
Weight loss is one of the most evidence-based non-operative treatments for knee osteoarthritis, particularly in those who are symptomatic. Every step we take places a load through the knee joint, and body mass increases that load. The forces can be as high as 3 to 6 times body weight, studies show.
Even a small amount of weight loss (5 to 10 percent of total body weight) can reduce the load. For instance, when you lose 10 pounds, you’re taking 30 to 50 pounds of pressure off each knee with every step.
This decrease in mechanical load also has an effect on cartilage biology, with less cartilage damage and reduced joint inflammation.
Sleep, Stress Management, and Daily Activity Tips
Daily habits apart from exercise and diet can also help relieve joint pain. A good sleep (7 to 9 hrs) is important; inadequate sleep is associated with lower pain thresholds and higher levels of inflammation, worsening symptoms of OA.
- Stress Management Tips: Mindfulness, yoga, breathing slowly, and resting on schedule.
- Sleep: 7 to 9 hours; bad sleep makes pain worse.
- Daily activities: Don’t stay in one place for too long (too much sitting or standing) and wear good shoes.
- When lifting, use your legs (bend your knees, keep your back straight).
Supplements and Diet
Glucosamine (usually 1500 mg per day) and chondroitin sulfate (around 800-1200 mg per day, sometimes not all at once) have been widely researched.
The meta-analyses suggest modest, inconsistent benefits for pain and function, especially for glucosamine sulfate (not hydrochloride) and chondroitin sulfate.
Glucosamine and chondroitin
- The evidence is variable: Some people find their symptoms improve; however, others don’t.
- Dosage: Typical doses are glucosamine 1500 mg per day and chondroitin 800-1200 mg/day, but speak to your healthcare professional.
- Warnings: May interact with other medications; begin with a test period and observe.
Collagen for a Healthy Joint
- Types: Types I and II collagen are the most common in supplements.
- Dosage: Stick to the product instructions; some protocols include 5–10 g/day.
- Building blocks: Support the cartilage matrix and joint stability.
Omega-3 fatty acids and Inflammation
- Food sources: fatty fish, flaxseeds, chia seeds, walnuts.
- Supplements: Talk to your healthcare provider about taking 1-2 g/day of EPA/DHA combined.
Anti-inflammatory Diet Foods
- Basic meal suggestions: Salmon with quinoa and greens; lentil soup with olive oil; veggie stir-fry with turmeric.
- Grocery list: Berries, leafy greens, oily fish, olive oil, nuts, seeds, whole grains.
Sun Exposure and Vitamin D Considerations
Vitamin D is important for bone and cartilage health. So, get some sun exposure or take supplements as recommended by your healthcare provider.
Hydrate and Lubricate
- Drink water and stay hydrated: Water is an essential component of healthy synovial fluid.
- Rest for at least a day after hard workouts.
- Apply heat or ice for pain management.
Is there a New Treatment for Knee Cartilage without surgery?
New treatments are constantly emerging. Stem cell knee injections, PRP (platelet-rich plasma), and next-generation biologics are areas of intense research.
Short note: ACI and MACI
These are sophisticated cellular therapies and involve operations.
They are not non-operative strategies, and they are here mentioned to provide an outlook.
The difference from non-operative modalities
Surgical (repair) versus non-surgical management has different implications for invasiveness, convalescence, and objectives.
Nonoperative treatment is for symptom control, and it supports cartilage health without any tissue excision.
When to consider Surgery and Non-surgical Approaches
Surgical treatment may be considered if non-surgical care does not adequately manage pain or function, or if the damage is severe.
However, get a plan standardized with a knee specialist BEFORE you decide.
FAQs about Knee Cartilage Repair without Surgery
Do non-surgical treatments work for advanced knee osteoarthritis?
These treatments may not reverse the damage caused by the injury, but they may reduce pain and delay surgery for some patients (e.g., weight loss + PT + HA injection).
How long before I see improvement with PRP or hyaluronic acid injections?
PRP: a few weeks to months; HA: usually a few weeks to a couple of months, based on how the individual responds.
Are there risks with stem cell knee injections or PRP?
Both procedures are usually regarded as safe when carried out with autologous cells in sterile conditions. Temporary risks that are common include infection, swelling, and allergic reactions.
Can lifestyle changes alone halt cartilage wear?
They may slow progression and lessen symptoms, particularly in conjunction with targeted therapy and exercise.
How should I choose between therapies?
Choice depends on personal goals, symptom patterns, and imaging findings. Add HA for mechanical symptoms/stiffness, consider PRP for inflammatory-mediated pain, consider stem cells for chronic synovitis, and use prolotherapy cautiously for signs of instability, and as always, weave in foundational lifestyle and supplement guidance.
Summary of Evidence
- PRP: There is moderate evidence to support short-term symptomatic relief in knee osteoarthritis; efficacy depends on preparation and injection protocol.
- Hyaluronic acid injections: Short- to mid-term relief (moderate evidence); duration of effect varies.
- Viscosupplementation: Same as HA injections, relief duration is traditionally 3-6 months from the injection, but a few special high-MW/cross-linked product reports longer periods of relief.
- Prolotherapy: Limited high-quality evidence; some patients experience better stability.
- PT results: Strong evidence exists that pain can be reduced and function improved.
- Stem cell knee injections: Preliminary results; more research is needed to determine whether there are long-term benefits.
A Clear Path for Knee Cartilage Repair without Surgery
- What you need to know: See a knee specialist, physical therapist, or orthopedist to talk about your options for non-surgical knee cartilage repair and to get a customized treatment plan.
- Develop a plan that includes non-surgical knee cartilage repair options, PT, and nutrition.
- Monitor progress. Use a pain scale, function scores, and activity tolerance to observe changes.
Monitor progress
- Pain scale: Are you improving? Rate your pain daily or weekly.
- Function scores: Monitor your ability to do everyday activities or certain things.
- Activity tolerance: Keep track of how long you can walk, climb stairs, or ride your bike.
Read also: Robotic Surgery Systems: Scope, Design, and Implications.
Final Thoughts: Knee Cartilage Repair without Surgery
The non-surgical treatments ease the symptoms and help maintain the cartilage. There’s no doubt they work for many people, especially if you start early and combine them with physical therapy, nutrition, and lifestyle modifications.
Non-surgical treatment for knee cartilage damage includes stem cell knee injections, PRP, knee injections of hyaluronic acid, and viscosupplementation.
Prolotherapy presents an alternative avenue to joint stability through ligament-based injection therapy.
In its focus on strengthening neuromuscular control and gradual progression, physical therapy for knee cartilage is similar to rehab for other knee injuries.
Quick glossary of terms
- PRP therapy knee: Knee injections with platelet-rich plasma to promote healing.
- Stem cell knee injections: Injections to influence the joint environment with stem cells.
- Hyaluronic acid knee injections: Injections to help lubricate the knee.
- Viscosupplementation: The injection of hyaluronic acid to restore or improve joint viscosity.
- Prolotherapy: Injection to promote tissue repair and stability.
- Physical therapy for knee cartilage: A rehabilitation routine to reduce discomfort.
- Anti-inflammatory foods: Diet to cure inflammation in joints.

In the emergency room, trauma bay, and oncology clinic, a quick and accurate read can modify treatment courses; reduce length of stay, and save lives. A CT scan reader offers a seamless workflow with precise diagnoses, powered by trusted software and the latest-generation artificial intelligence (AI). In this article, you will learn what a CT scan read is, what it’s used for, and how AI contributes to the process of reading CT scans.
What Is a CT Scan Read?
Computed tomography (CT) scan reader combines the expertise of the human radiologist with advanced tools to provide fast, decisive interpretation. It includes efficient workflows, high-performance image processing, and, when applicable, AI support for triage, quantification, and notification of abnormalities.
The idea: Turn around dependable reports with the least delay possible so caregivers can make decisions with full confidence.
The ring-shaped part of the scanner rotates around the patient, emitting X-rays to produce axial images, which can be converted into coronal and sagittal images with no additional radiation exposure.
These T-shaped (MPR) images show you things that you can’t appreciate on flat films, so that makes CT crucial for finding hemorrhages, fractures, pulmonary emboli, solid tumor masses, and vascular abnormalities.
Contribution to diagnosis of axial, coronal, and sagittal views:
- Axial, coronal, and sagittal views each have their advantages and disadvantages in evaluating pathology.
- Axial: Horizontal slices give a “block” view and are the best slices for detecting acute pathology.
- Coronal: Frontal plane sections are useful for evaluating the relation of structures over larger distances (e.g., chest or abdomen).
- Sagittal: Laterally obtained images provide side views. Depth relationships are essential and very useful for spine, brain, and pelvis examinations.
Why CT is preferred in trauma, oncology, and emergency care:
- Speed: Images are captured and interpreted quickly.
- Sensitivity: Identifies subtle fractures, hemorrhage, organ damage, and mass effect.
- Versatility: Can examine bone, soft tissue, and contrasting vascular structures.
How Long Does It Take to Read a CT Scan?
Reading a CT scan is not a single-step procedure. Turnaround times are influenced by several factors, such as:
Scan Protocol
Full multiphase or combined protocols are more time-consuming to read than focused studies. A simple, single-phase chest CT for infection may be interpreted more rapidly than a multiphase abdominal study or a dedicated contrast-enhanced vascular protocol.
Patient Status
You need to triage and report on unstable patients faster to direct immediate intervention. When working in an emergency, radiologists focus on findings with an immediate management effect, such as a ruptured organ, a collapsed lung, or heavy bleeding.
Radiologist Workload
Immediate cases can increase the turnaround time. They can also reduce the speed of each reading.
AI Aids
Automated detection and pre-reading analyses can help radiologists understand data faster. AI tools can flag critical findings and sort images and studies.
What to Expect in Various Situations

Emergency Department CT
The focus in emergencies is on the speed of triage and the detection of critical findings. Turnaround time ranges from minutes to a few hours.
Inpatient imaging
Inpatient studies may be scheduled and reported within hours in case of an acute change in the patient’s condition.
Outpatient CT
In the case of routine outpatient examinations, reports could be delayed often by hours and, in some cases, by a day. It depends on the number of examinations to be reported and the complexity of the protocols.
How to Control Interpretation Speed
Workflow design
In radiology practices, prioritizing rules, dedicated emergency reading teams, and matching workflows reduce delay.
Technology
PACS, advanced viewers, and AI-assisted pre-reading may enable the review, mostly in high-volume facilities.
Communication
Quick, clear communication of critical findings is necessary, sometimes through a notification system, even before the full report has been completed.
What can patients do?
Ask about the protocol.
Ask about the type of scan and whether it is a multiphase or a focused protocol. Now you understand why the CT scan read might take longer.
Discuss urgency.
If your condition is changing, please inform your care team so they can re-evaluate the prioritization.
Follow result timing recommendations.
You don’t have to get into all the technical aspects, but knowing that reading times are different for every protocol, patient condition, and workload can help you manage your expectations.
Typical ranges for emergency vs. routine reads
Emergency reads
Preliminary report generated within minutes.
The full report is usually ready in 15-60 minutes, or up to an hour, depending on the complexity.
Routine reads
Those that are extensive can require several hours.
It is not uncommon for final reports to be received within 24 hours.
Models that support read times (uses, features, and benefits)
AI-powered detection and triage solutions
Applications: Identify critical findings (e.g., hemorrhage, pneumothorax) early; triage cases for priority reading by radiologists.
Features: Detection of anomalies, workflow automation, and PACS integration.
Benefits: Enables speedy initial readings, and it assists in caseload balancing.
AI-driven pre-reading platforms
Application: Pre-screen scans to generate a preliminary read for radiologist confirmation.
Features: Probabilistic lesion scoring, ROI highlighting, structured reporting templates.
Benefits: Decreases verification time, increases consistency in emergencies.
Voice-enabled or dictation enhancement
Applications: Report generation from narration. Generate reports as the radiologist narrates and converts them into reports.
Features: Real-time transcription, voice commands, and a link with imaging findings.
Benefits: Reduces time spent on documentation and less typing.
Tools for quantitative and imaging analysis
Applications: Lesion size quantification, organ volumes, or perfusion parameters for support analysis.
Features: Automated calculations, tracking trends between studies, quality assurance checks.
Benefits: Objective information is obtained faster, allows monitoring, and improves the precision of reports.
Focused problem-based reading aids
Application: Leads the radiologist to the answers to clinical queries (e.g., trauma, stroke).
Features: Checklist-style reminders, protocol-based layouts, compatibility with clinical notes.
Benefits: Increases efficiency for focused studies, limits overlooked findings, coordinates with emergency workflow.
A CT Reading Workflow and Useful Tools
The standard diagnostic process includes four steps:
- Image acquisition
- Secure transmission to a picture‑archiving and communication system (PACS)
- Interpretation by a competent reader
- Final report generation
Common Challenges of CT Scan Read
Motion artifacts, poor contrast timing, and anatomical variants that resemble disease.
Mitigation techniques include technologist-driven protocol checks, real-time dose monitors, and application of sophisticated reconstruction algorithms (e.g., iterative reconstruction and metal-artifact reduction).
AI is now integrated within this workflow as a second reader: it can alert for suspicious nodules, calculate lesion volume, or triage studies for critical findings, freeing the radiologist to spend cognitive effort on the application where it is most needed.
Is There an AI That Reads Your CT?
Yes, several AI products with the CE mark and FDA clearance support CT reading. These algorithms can identify intracranial hemorrhage, flag pulmonary nodules, calculate coronary calcium scores, and detect vertebral fractures.
However, they are support tools; the radiologist retains final responsibility.
Safety aspects comprise ‘ensuring algorithm transparency, monitoring for drift (inter-institutional, inter-scanner), and continuous stringent validation with the use of diverse patient cohorts. ‘
And ethically, departments need to receive informed consent when AI has a role in clinical decision-making and comply with privacy legislation and regulations related to algorithms.
CT Scan Read Solutions (Medical Professionals & Radiologists)
Tools for Diagnostics (Paid Tools)
RadiAnt DICOM Viewer (Windows)
It has an advanced MPR, 3D volume rendering, and hanging protocol customization. This is a reliable clinical DICOM viewer.
Features:
- Robust MPR and fusion
- Rich plug‑in architecture for research
- Routine report generation
- Enterprise and Institutional Platforms
Sectra PACS CT Scan Read
This scalable vendor-neutral architecture allows smooth integration of CT, MR, ultrasound, etc. The Sectra PACS provides high availability and role-based security.
Features:
- Visage Imaging
- Collaborate among radiology, oncology, and surgery
CT Scan Read Solutions for Personal & Educational Use
Web-Based (No Installation)
IMAIOS DICOM Viewer
- Drag and drop within all modern browsers
- Suitable for quick case review, teaching sessions, and remote consultancy
ViewMedicai Free CT Viewer
- Access to active patient studies from any web browser plus
- Use basic measurement tools.
- Allows HIPAA-compliant sharing of studies
Desktop Programs for Mac, Windows, and Linux
Horos CT Scan Read
The best free 64‑bit DICOM viewer for macOS with MPR, 3D rendering, and DICOM‑net features is truly free open-source software without any licensing fees.
MicroDicom CT Scan Read
A simple Windows DICOM viewer with basic windowing (WL/WW, zoom, pan, and flip), annotation, and export features is suitable for self-study and small practices.
How to Find the Best CT Scan Reader
DICOM compliance, powerful MPR and 3D visualization, integration with PACS or VNA, role-based access control, and compliance with local regulatory requirements such as FDA 510(k) or CE marking should be considered first.
Best Pick
RadiAnt Viewer
Applications: Standard radiology reading, fast multiplanar reformats, elementary 3D rendering.
Features:
- DICOM-compliant
- Lightweight installer
- Customizable toolbar
- Built-in measurement tools
Benefits:
- Low cost
- Fast startup
- Little training needs
- Good community support
Best Pick:
OsiriX MD CT Scan Read
Benefits:
- Subspecialty oncology follow-up
- Advanced quantitative analysis
- Research-grade image processing
Features:
- FDA-cleared 510(k)
- Multi-GPU acceleration
- Wide plugin architecture
Best Model:
3D Slicer
Uses: Academic case-based teaching, image-guided therapy planning, volumetric segmentation research.
Features:
- Open-source platform
- DICOM import/export
- Extensible modules for MPR
- 3D rendering, and AI integration
Benefits:
- Zero licensing fee
- Active developer community
- Cross-platform compatibility
- Extensive documentation
Considerations for the Medical Professional Section
Diagnostic accuracy, speed of workflow, and compliance with regulations should be considered.
Invest in a viewer with full-featured MPR/3D tools, strong PACS/VNA integration.
Focus on role-based access to protect patient data, and the ability to turn around cases faster.
For Prospective Students and Educators
Choose free or web‑viewers with user‑friendly UIs, annotation libraries, and cross‑platform support (iOS, Android, Windows, and Mac).
They make sharing easier, and they remove licensing constraints.
Administration Matters
Consider enterprise scalability, total cost of ownership, vendor support, and oops prevention and deterrence capabilities.
So, a product that supports your requirements in these areas is suitable for long-term regulatory and operational effectiveness.
How To Improve CT Scan Read Turnaround Time
Standardized reading protocols
Use protocol templates for head, chest, abdominal (contrast), and trauma CT.
Turn on auto presets for windowing and labeling and reduce cognitive load.
Preset workflows
Insert protocol templates in the PACS to auto-pop the appropriate series and recons.
Use standardized naming conventions to guide technologists and radiologists through procedures step-by-step.
Keyboard Shortcuts & Automated Measurement
Assign keyboard shortcuts for navigation
Use automated length, density, and volume measures to reduce interobserver variability.
AI‑Assisted Alerts
Enable AI triage for large hemorrhage, pneumothorax, and midline shift and alert on those instantly.
Define confidence levels to reduce false alarms and to enforce radiologist verification before acting.
Continuous Training & Education
Conduct bimonthly case-review meetings, didactic sessions, and simulation workshops.
Perform calibration routines on known phantom images to ensure accuracy of measurements.
Peer Review / Double-Reading
Introduce a second reader for complex trauma, oncologic follow-up, or equivocal findings.
Promote teaching-file conferences in which discrepancies are resolved by consensus.
Bringing Best Practices Together
Integrate standard protocols, shortcuts, AI alerts, and ongoing training into a single workflow.
Track turnaround and diagnostic performance indicators to inform ongoing improvement.
FAQs on CT Scan Read
What is a CT scan read?
An imaging technique that uses rotating X-ray beams and computer reconstruction to obtain detailed cross-sectional images of the body.
What is a CT scan used for?
It is used to assess trauma (head bleeding, fractures), oncology (tumor staging, metastases), vascular disease (CTA, pulmonary embolism), abdominal pathology (appendicitis, diverticulitis), and to guide interventional procedures.
How long does it take to read a CT scan?
In emergencies, read times range from 2 to 5 minutes for focused scans; in routine multiphase exams, 10 to 15 minutes, depending on the complexity of the protocol and the workload of the radiologists.
What are some good reading practices for a CT?
Use a second reader who uses a standardized protocol, shortcut keys, automated measuring tools, and alerts from AI as well. Be a student and continually learn.
Is there an AI that can read CT scans?
AI applications can detect hemorrhages, nodules, fractures, and lesions in CT scans; however, these applications are decision aids and require radiologist oversight and regulations.
Read also: Types of CT Scanners: Features and Buying Tips
Final Thoughts on CT Scan Read
Quick, accurate CT interpretation is still a vital component of modern patient care, especially in the most urgent of medical fields.
When you select a reader compatible with the institution’s workflow, such as a high-end workstation, enterprise PACS, or a free web-based tool, that can diagnose and improve patient outcomes.
Take note: The future of CT reading is not to replace the expert eye but to supplement it with technology that reduces repetitive tasks and highlights important findings.
Disclaimer: This guide offers empirical support for faster and more accurate CT interpretations. And it’s for educational purposes.
When a critically injured patient arrives at the emergency department, the medical team do all they can to stabilize the person, and one of the things they use is the emergency steroid ampoules. These tiny vials have powerful anti-inflammatory and anti-allergic properties necessary vital for trauma treatment.
In trauma, some patients may have a severe inflammatory response, an allergic reaction to blood products, or adrenal insufficiency. However, with the appropriate steroid ampules, doctors can intervene immediately.
This guide covers all aspects of emergency steroid ampoule procurement for trauma centers.
How Emergency Steroid Ampoules Work
Emergency steroid ampoules have several purposes in trauma care. Its primary function is to reduce inflammation from severe injury. Certain Injuries can trigger irreparable inflammation that can damage internal organs.
The ampoules are also used where there is a sudden allergic reaction. Trauma patients receive blood transfusions, antibiotics, or other drugs quickly. Some sufferers are allergic to these medications.
Also, certain trauma protocols, steroids support hemodynamic stability. Patients on long-term steroid therapy, adrenal crises may occur during trauma.
What to do when timing and delivery are most important. Intravenous infusion produces the quickest results. It places the patient on life support within one to two minutes. But when IV infusion is difficult, doctors can use intramuscular infusion.
What’s Inside Steroid Ampoules
The active ingredient in most emergency steroids can be any of these: Hydrocortisone, Dexamethasone, Methylprednisolone. Each steroid has its potency and half-life.
Essential Emergency Steroids in Trauma Care
- Methylprednisolone Sodium Succinate (Solu-Medrol): A high-dose IV steroid administered within 8 hours of acute spinal cord injury; minimizes inflammatory injury to the cord; given as a single high-dose bolus.
- Dexamethasone: Potent anti-inflammatory; first line for anaphylaxis; reduces airway edema rapidly; administer IV or IM for rapid relief.
- Hydrocortisone: IV use; indicated in shock unresponsive to conventional therapy; source of cortisol in states of diminished adrenal reserve; indicated in acute stress.
Trauma centers maintain a narrow window to stop the after-effects of injury. Doctors use any these active ingredients to melt away in the bloodstream. These compounds reduces inflammation, stabilize blood pressure, and protect vital organs.
The three substances, methylprednisolone, dexamethasone, and hydrocortisone, constitute the basis of the rapid steroid armamentarium.
Methylprednisolone sodium succinate
Commonly referred to as Solu-Medrol, it travels directly to the injured spinal cord. Trauma teams administer a single 30 mg/kg IV bolus dose within eight hours after injury, preferably as soon as possible.
The drug interrupts the inflammatory cascade, reduces edema, and preserves neurologic function. Delivering the drug early is vital; doses given late have little effect.
Dexamethasone
This has a strong anti-inflammatory effect for acute allergic reactions. And when anaphylaxis occurs, 1–10 mg is administered by IV push (0.5 mg/kg/dose to 1 mg/kg/dose up to 10 mg every 4–6 hr).
The drug reduces airway inflammation and helps patients breathe within minutes, and it also decreases the likelihood of late-phase responses. Because it works rapidly, dexamethasone is sometimes used in place of epinephrine if a rapid airway obstruction continues.
Hydrocortisone
A usual dose is a 100 mg IV push, repeated or continuously infused until the blood pressure is stabilized. This steroid acts like the cortisol produced by the body and that helps the adrenals during high stress. It should be given early to prevent organ dysfunction.
Tight timelines govern when trauma teams can give these steroids. Methylprednisolone therapy must begin within 8 hours of injury; earlier is better.
Dexamethasone is administered immediately. Hydrocortisone is usually reserved for refractory hypotension but should be given as soon as traditional vasopressors do react of most immediately.
Emergency Medical Steroid Ampoules for Trauma Centers
There are different kinds of emergency steroid ampoules used by trauma centers. Sorting is done mainly by active substance, strength, and size.
Single-dose ampoules
These hold volumes for use only once, eliminating the hazard of cross-contamination even if the rubber stopper is punctured several times. They are great for rapid use in a resuscitation.
Multi-dose vials
Many health institutions don’t use the multi-dose formats because of infection control.
Sterile vs. non-sterile formulations
There are non-sterile versions, but these are for veterinary or research applications only.
Variations in concentration influence dose size. The standard hydrocortisone is 100 mg/ml. Dexamethasone is available as 4 mg/ml or 10 mg/ml solutions.
Methylprednisolone is mostly available in concentrations of 40 mg/ml or 125 mg/ml.
Why Trauma Centers Rely on Ampoules
Quite fast
Speed is the main benefit. Ampoules need not be reconstituted, mixed, or have any other supply used apart from the usual syringes and needles.
Efficient
Dependability is very important in trauma. Each ampoule contains a single predetermined dose of medication. So, miscalculations or errors preparing the dose is limited. The preparation is stable until used.
Follows medical standards
When you find your entire trauma bay with the same emergency steroid ampoules, your staff knows exactly what they have and how to use it. This consistency proves critical in high-stress resuscitations.
Storage
Ampoules occupy very little space. They are also used on crash carts, trauma kits, and pull bags. Many preparations are stable to temperature variations and can be used in some places within the trauma center.
These are the factors that have a direct impact on patients. Available at the right time, appropriate steroid ampoules permit quick treatment of anaphylaxis, adrenal crisis, and aggressive inflammation.
Buying Guide Essentials for Trauma Centers
Regulatory and Compliance Considerations
Procurement teams must ensure that products have the proper approvals. In the United States, the FDA is required to approve pharmaceutical products. Similar bodies in other countries oversee approval. Always make sure that the emergency steroid ampoules you purchase have the correct marketing authorization.
Lot tracing
A batch should be traceable from the manufacturer to the patient. This is vital in the case of a recall. The supplier should supply lot information with each shipment.
Inventory system
Many facilities have automated inventory systems that alert workers when products are approaching the expiration dates. They can send the remaining items back to the manufacturers. But this happens when there is an established elation.
Quality and Supplier Assessment
The reputation of the manufacturer is also important. Research a company’s history, customer feedback, and industry standing. Find established pharmaceutical companies with a successful history.
“Good Manufacturing Practice” means quality commitment. Certified GMP suppliers will have consistent production standards, proper documentation, and regular inspections. Ask suppliers if their products are GMP-certified.
Recall history indicates potential quality problems. Regular recalls indicate manufacturing or quality control problems.Also, search for suppliers with ISO certifications or who undergo regular third-party audits..
Product Specifications to Verify
Verify the active ingredients to make sure you get exactly what you ordered. Make sure you get the specific steroid, concentration, and volume.
Confirmation the dosage
Study the fill-volume specification carefully. Ensure stated volumes correspond to actual volumes within an allowable tolerance. The contents should be clear, free from any particulates, discoloration, or floating substances.
Storage and handling instructions
Some steroid ampoules are to be stored in a refrigerator at 2-8°C. Others are stable for storage at room temperature (up to 25°C). Understand the needs of your product and supply suitable storage.
If you don’t have air conditioning/temperature control in that environment, get products that can tolerate those conditions.
Whether they are really usable is determined by your ability to access them in the trauma bay. Keep the products within reach of the responders. Possibly in a wall holder near, on, or in the crash cart or in a trauma box.
Inventory and Risk Management
Determine the appropriate par levels with the addition of safety factors to past usage data.
Have the first-expired-first-out method applied to avoid any waste product. Perform systematic checks to ensure that the oldest stock is used first.
Supplier failures are dealt with in contingency plans. Designate alternative suppliers who can provide the same goods on short notice following disruption of your primary supplier.
Contingency sourcing arrangements are also useful when supplies are limited or when credit availability is stretched. Ideally, you should build relationships with multiple suppliers.
Compatibility with Clinical Protocols
Make your purchases consistent with trauma activation protocols. Verify that the concentration and volume of the product are compatible with the protocol. Liaise with other services. Emergency physicians, trauma surgeons, pharmacists, and nurses.
Cost Considerations
The cost of ownership is more than the purchase price. Include handling charges, storage fees, waste removal, and your time.
Negotiated volume discounts are typical in combined product agreements. If possible, negotiate bundled contracts for multiple product categories.
Strategies to reduce waste cut unnecessary costs. Correct rotation, correct par levels, and accurate forecasting all help keep the cost down.
How to Assess Suppliers and Products
Check the status
Shortlisting needs to be based on research. Check the regulatory status. Don’t contact vendors not dully licensed and certified.
Delivery period
Reach out to current customers and inquire about their rates, and delivery time. Chronically delayed deliveries create patient safety concerns. Inquire with prospective suppliers about any adverse events related to their products. Find out how they managed such incidents.
Buy small
Order samples to test for packaging integrity, ease of opening, and readability. Let clinicians evaluate usability in the simulated scenarios.
The review of documentation finalizes the evaluation. Ask for MSDSs, COAs, certificates of sterility, and current expiration dates. Poorly documented information is a red flag.
Pilot, not once, but twice. Run a test batch in one department. Receive feedback from users. This kind of testing can expose problems that wouldn’t arise in laboratory tests.
Tips for Trauma Center Development
There should be uniform terminology in all of the documentation, ordering system, and clinical records. It prevents confusion and reduce administrative errors.
Labeling concerns are warranted. Every ampoule should be uniquely identified with the name of the drug, concentration, volume, expiration date, and lot number. Use labeling systems that conform to regulatory requirements…but don’t forget they’re in a high-paced trauma environment.
Integration of EMR is a boon to keeping track. Integrate your EMR with your pharmacy dispensing systems. This allows for the automated documentation, inventory management, and expiration notifications.
Training of personnel is multifaceted. The staff needs to know how to store, handle, and dispose of it. Consistent performance is maintained through periodic re-evaluation of competency.
Disposal practices need to be well thought out. Containing pharmaceutical waste: used and expired ampoules. Dispose of in accordance with environmental regulations and institutional policies.
Final Thoughts
Steroid ampoules for emergencies have their importance in trauma care. How they work, which informs the right product choice on the procurement side. When you know which contents to choose from—hydrocortisone, dexamethasone, or methylprednisolone—you can make an educated buying decision.
There are several types, each designed for different clinical applications. Trauma centers count on ampules to provide the speed, reliability, and standardization that saves lives.
Some buying considerations are regulatory compliance, quality assurance, product specifications, storage and handling requirements, inventory management, alignment of protocols, and cost-related issues.
In addition, make sure that you verify potential vendors. Review samples, and check their website.
-
 Uncategorized7 months ago
Uncategorized7 months ago6 Best Heatmap Plugins – I Test, Review and Compare
-
 Diagnostic & Hospital Equipments6 months ago
Diagnostic & Hospital Equipments6 months agoWhat Are Medical Devices? Types and Uses
-

 AI in Health care6 months ago
AI in Health care6 months agoRemote Patient Monitoring in Modern Healthcare
-

 AI in Health care4 months ago
AI in Health care4 months agoDigital X-ray vs. Film X-ray: Which is better?
-

 Review and guides6 months ago
Review and guides6 months agoCPAP Machines Buying Guide: The Best Models Doctors Don’t Recommend
-
 Diagnostic & Hospital Equipments4 months ago
Diagnostic & Hospital Equipments4 months agoDEXA Bone Density Scanning: What You Need to Know About Bone Health
-
 AI in Health care6 months ago
AI in Health care6 months agoAI in Medical Imaging: What is Coming Next
-

 Diagnostic & Hospital Equipments4 months ago
Diagnostic & Hospital Equipments4 months agoPET Scan Machines: Understanding the Technology, and Usage